
85% of Patients Never Make It Into Clinical Trials. We Built the Tool to Change That.
Partnered with Mayo Clinic physicians to design an AI-powered trial-matching platform that tackles the #1 barrier to medical innovation: patient enrollment failure.

Project Overview
Clinical trials are essential for advancing cancer treatment, yet 85% fail to recruit enough patients on time. This bottleneck doesn't just delay life-saving therapies—it costs trial sponsors between $600k–$8M per day in operational burn.
Our AI-powered platform, Clinspire, was designed to solve this dual challenge. By replacing dense medical forms with an accessible, conversational interface, we created a system that guides patients with empathy while optimizing enrollment velocity for the business.
The Challenges


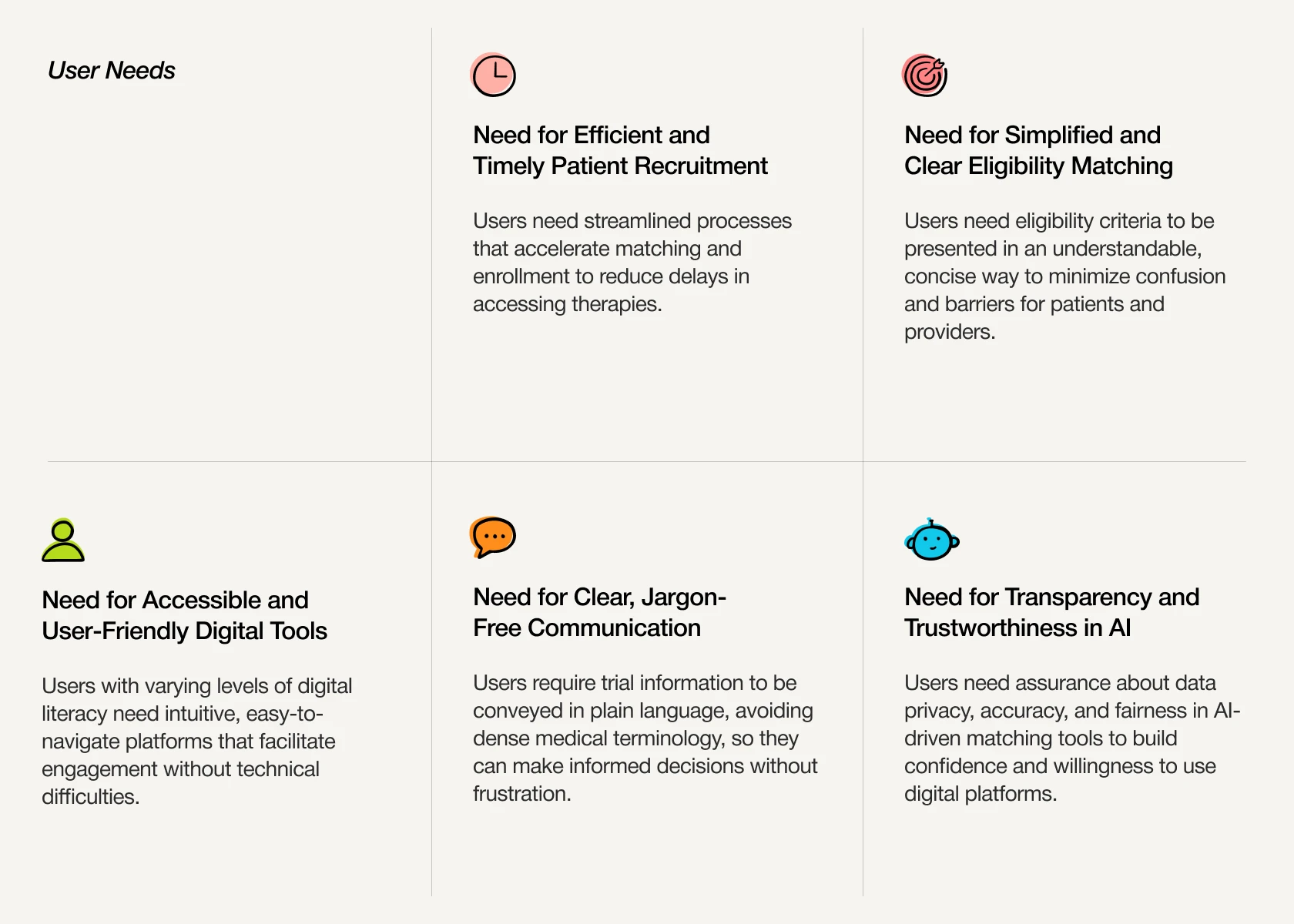
User Needs
Business Goals

The Roadblock
Our biggest constraint was that Mayo Clinic’s privacy policies prevented direct access to patients. To adapt, we collaborated closely with their clinicians and engineers instead. This pivot turned a limitation into an advantage, allowing us to uncover patient pain points and critical workflow bottlenecks directly from the provider’s perspective.

Research Insights
To diagnose the 85% failure rate, we triangulated data from Affinity Mapping (to isolate cognitive friction) and Competitive Analysis (to identify market gaps). Targeted Interviews then confirmed the root cause: the bottleneck wasn't a lack of patients, but a lack of process clarity.

The Aha Moment
Clinician interviews revealed that trial-matching issues stemmed from the patient side unclear histories, inconsistent terminology, and incomplete data.
The initial design attempted to address both patient and clinician simultaneously, which led to a less focused experience.
We realized the root problem wasn’t matching, it was the patient onboarding experience.

Ideation
We mapped the patient journey to pinpoint friction driving abandonment-especially around medical jargon and complex eligibility-turning vague drop-offs into clear design opportunities.

Initial Wireframes
Based on user flows and identified friction points, I created initial wireframes.

Final Designs
Building on the validated wireframes, I refined the high-fidelity UI to establish patient trust. I prioritized a clean visual hierarchy that helps users instantly toggle AI simplification, verify their eligibility status, and complete the enrollment flow without cognitive fatigue.



We organized eligibility criteria into clear sections Met, Unmet, and Need Review, so users could easily understand their status and progress, effectively reducing confusion.

By simplifying medical jargon with AI and presenting clear eligibility criteria, we make information accessible to users with varying health literacy, helping them quickly understand their status.

Users can opt for AI-guided onboarding, making the process easier for those who are fatigued, visually impaired, or prefer not to complete forms manually.

Testimonials and community insights can help users trust the platform; future enhancements like transparent AI explanations, privacy assurances, and human oversight will further ease concerns.
Final Prototype
Outcomes
Clinspire’s design is expected to drive the following positive outcomes, making clinical trial participation more human-centered and equitable.

My Learnings

Future Enhancements
Due to strict medical privacy policies, I could not interview patients directly during this phase. My top priority for the next iteration is to bring real patients into the research loop, ensuring we validate our design decisions against their first hand experiences and emotional needs.

